We discuss the needs of hematooncology patients with Prof. Krzysztof Giannopoulos.
Hematooncology: Immunotherapies are changing the reality for patients

Published July 3, 2024 10:26

What is characteristic of the therapeutic processes in hematooncology is that new solutions, new molecules are constantly emerging. The situation of treated patients is changing, but also their needs. We are seeing a great development precisely in therapies, and there are now some that have a new mechanism of action. Please tell us more about this, about what this mechanism is and how this is changing the situation of hematooncology patients?
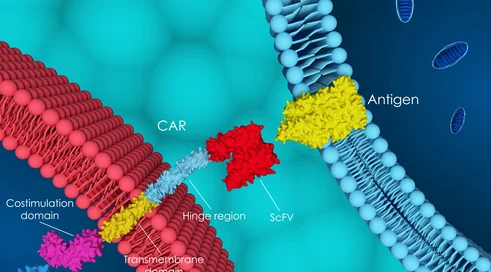
The question is very timely, as the European Society of Hematologists conference, where current research and changing standards of therapy were summarized, ended not long ago. Indeed, immunotherapies, for that is how broadly we can define this new group of therapeutics, are changing the reality for patients with plasma cell myeloma, chronic lymphocytic leukemia and lymphomas. In acute myeloid leukemia, this development is still slow. But let's get back to immunotherapies, because they do indeed seem to be making breakthroughs. The director of hematology and oncology, at one of Europe's largest hospitals in Charite, said that 35 to 40 percent of all patients are already receiving immunotherapy. That is, you can see that we are seeing chemotherapy being measured and that there is indeed a shift toward immune therapies. We have two main streams of development of these therapies. The first is CAR-T technologies, which in Poland are already reimbursed in lymphoma indications, in aggressive lymphomas. Also, in acute lymphoblastic leukemia there is also a lot going on. These CAR-T therapies are being modified and often already manufactured in centers that administer these therapies, as well as not necessarily the T-lymphocyte being used for the therapy, but, for example, NK lymphocytes, which also have some benefit from this therapy. On the other hand, the second area, which is developing in parallel, and in some indications seems to be even ahead of CAR-T technology, are the dual-specific or bispecific antibodies. These are off-the-shelf therapies, also we don't have to generate them, unlike CAR-T technology. The moment a patient requires treatment, it is a ready-to-use so-called off-the-shelf therapy that can be given directly to the patient. In a nutshell, these are bispecific therapies, that is, these are monoclonal antibodies produced by genetic engineering methods that recognize both an immune system cell and a cancer cell, such as a lymphoma cell. There is such a physical approximation, but we don't mean that, only that it is a certain mimicry of the way the immune system works. A cytotoxic lymphocyte, being near a cancer cell, recognizes it as foreign and produces a cytotoxic response, getting rid of these abnormal cells. We can see that, on the one hand, this is a therapy that targets abnormal cells, and on the other hand, it is a very specific therapy using the immune system. In Poland, we have good news - as of July 1, the Ministry of Health has included mosunetuzumab in reimbursement. This is the first dual-specific antibody that will be used in the treatment of difficult cases of lymphoma nodosa. Also, our previous experience with blinatumomab shows that indeed these therapies can already be safely administered in Polish centers. But we are waiting for more. And asking the experts of the Polish Society of Hematologists and Transfusionists about the greatest need, out of the 10 therapies needed, as many as 5 were dual-specific antibodies, and even so, these were not all listed. I hope that this first reimbursement is the beginning of the era of immunotherapy and the availability of this therapy in Poland both in aggressive lymphomas and in plasmocytic myeloma, because there, too, three therapies are registered and waiting for reimbursement decisions.
How will the situation for patients change once these new therapies are available?
These are not therapies that are a single treatment. We do, however, see them as a therapeutic sequence. As we improve the first and second lines of treatment, there are increasing challenges as to what to do in relapsed cases or in cases of therapy resistance. This is certainly an unmet medical need. This is the most effective therapy for this group of patients. Because these patients are already often resistant to chemotherapy. It is also a therapy that is relatively better tolerated by patients. Although here we have to learn as hematologists such unusual toxicities. Because it's not like in chemotherapy, where the biggest problem is deep cytopenias and infections, here they also happen, but they have a slightly different dynamic, because we are dealing with exploiting the immune system.